General Testing InformationPharmacists are Part of the Testing Solution
The complete letter regarding guidance from HHS can be found here: Declaration Under the PREP Act for Medical Countermeasures against COVID-19:
What Are We Testing for and What Types of Tests Are Available? There are two types of tests that are available for COVID-19 testing: viral tests and antibody tests. Viral Tests or Diagnostic Tests
CDC Testing Overview: FDA Testing Overview: FDA FAQ on Testing for SARS-CoV-2:
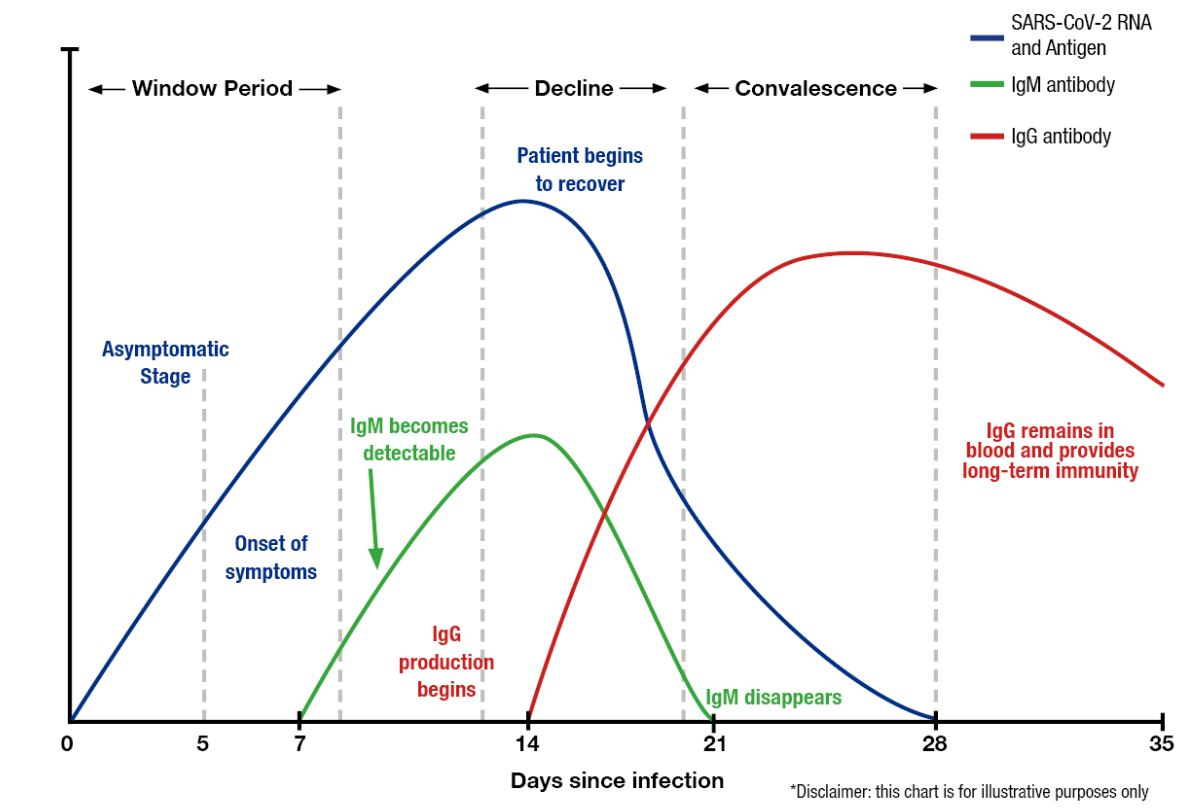
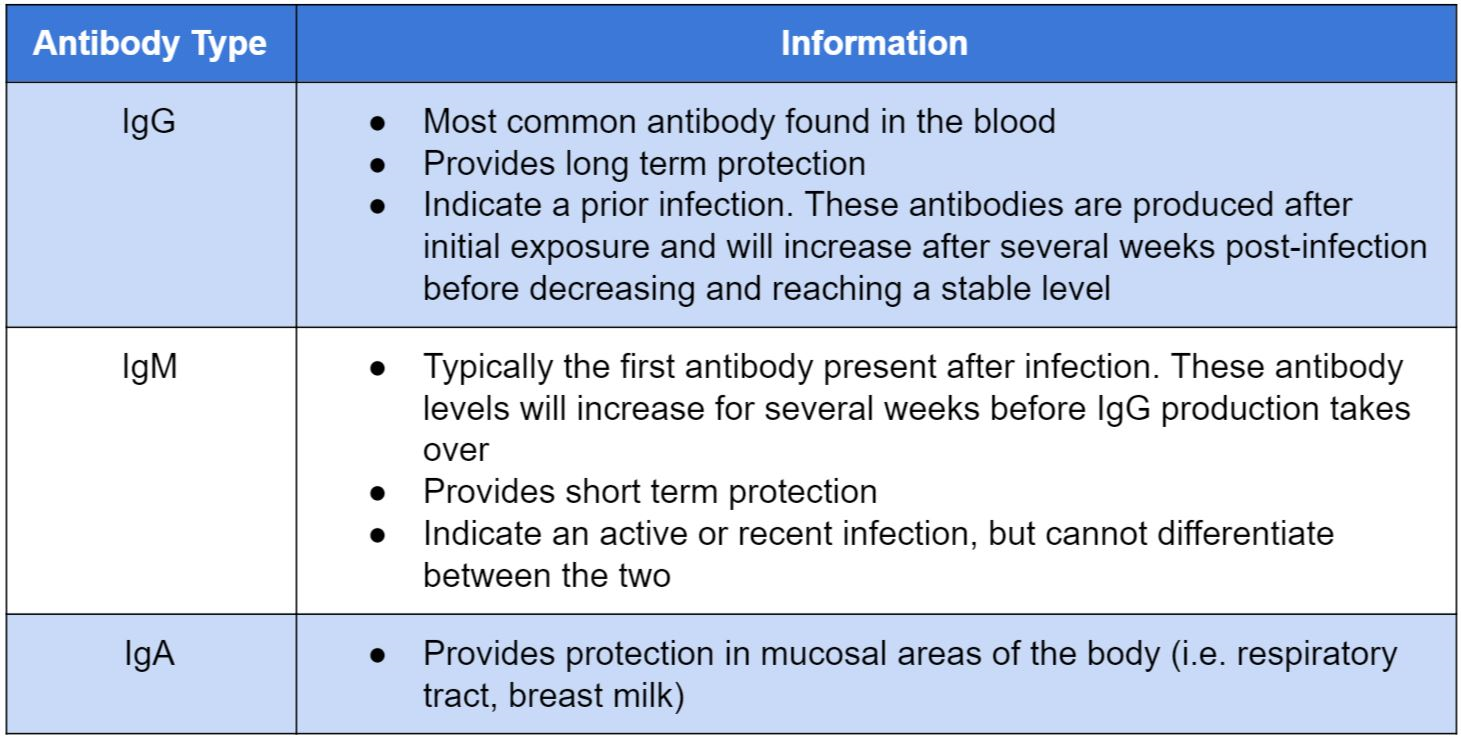
Serology Tests for Antibodies Antibody tests are a type of serological test used to check a blood sample for antibodies specific for SARS-CoV-2. This type of testing can show if someone has been previously infected with COVID-19, but should not be used to detect a current infection. After infection, it may take 1-3 weeks before antibodies are present in the body. Types of antibodies that may be tested for include IgG, IgM, and IgA. Enzyme-linked immunosorbent assay (ELISA) and lateral flow rapid tests are serology tests that can be used to test for COVID-19 antibodies. Antibody testing is important for assessing population exposure and helping medical professionals to better understand the immune response towards COVID-19. Additionally, it may be useful in determining individuals who can donate blood containing COVID-19 antibodies, which is one potential treatment under investigation. Lauer, S. et al., 2020. The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application. Annals of Internal Medicine. Antibody information:
Interim Guidelines for COVID-19 Antibody Testing:
Understanding Test Performance Sensitivity and specificity help to measure the validity of a test, or the extent to which a test measures what it is supposed to measure. Sensitivity is the ability of a test to correctly identify those with the disease, or the true positives. Specificity is the ability of a test to correctly identify those without the disease, or the true negatives. Sensitivity and specificity are inversely related. This means as sensitivity increases, the specificity decreases, and vice versa. It is important to be aware of the sensitivity and specificity of any tests your pharmacy chooses to administer in order to know how confident you can be in the results of those tests and whether subsequent additional testing is required. For viral tests, the timing of sample collection is important to achieve maximum test sensitivity. The sample should be collected from infected patients at the onset of symptoms for highest test sensitivity. If a patient is tested while they are infected, but not yet showing symptoms, test specificity will be increased, while sensitivity will be decreased. For antibody tests, there is no sensitivity within about 7 days after a patient is infected due to the time that it takes for antibodies to form and become detectable in the blood. Once IgM and IgG antibodies begin to form in response to a COVID-19 infection, the sensitivity of an antibody test increases, while the specificity of the test decreases. When there is no recognized clinical reference standard test for a disease, you can evaluate the performance of a test using positive percent agreement (PPA) and negative percent agreement (NPA). These are both measures on how often a new test agrees with a non-reference standard. It is important to note that agreement does not mean the test is correct, and agreement of a test to a standard can change depending on the prevalence of a disease. Although no test is 100% accurate, it is important to know the performance standards of each type of COVID-19 test for appropriate patient management. For viral diagnostic tests, antigen tests are known to be less sensitive than molecular tests. However, antigen tests are very specific for COVID-19, which minimizes the risk of a false positive. The EUA authorized serology test performances can be found at the following link: (https://www.aruplab.com/news/4-21-2020/How-Accurate-Are-COVID-19-Tests) Understanding Test Results For molecular and antigen viral diagnostic tests, a positive result means that the patient has COVID-19 at the time of testing. A negative result from a viral diagnostic test means that the patient does not have COVID-19 at the time of testing. According to the FDA, since antigen tests are less sensitive than molecular tests, negative results from an antigen test should be considered presumptive. See the first CDC link below for updated guidance on whether confirmatory testing with a molecular test is necessary to rule out a false-negative result. For antibody tests, a positive result means that the patient has previously been exposed to COVID-19, however, this type of test is not conclusive for a current infection of COVID-19. A negative result from a serology test means that the patient has never been exposed to COVID-19 and does not have antibodies for the virus. It is possible that an individual will not develop antibodies following infection. There is currently not enough evidence to determine how long antibodies to COVID-19 will help protect a previously infected person from becoming infected again. (https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antigen-tests-guidelines.html)(https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antibody-tests-guidelines.html)
Important Legal and Regulatory Frameworks FDA Emergency Use Authorization (EUA)
There are four criteria that must be met in order to enact an EUA during an emergency. Those criteria include: serious or life-threatening diseases or conditions, evidence of effectiveness, risk-benefit analysis, and no alternatives available. Once the emergency has passed, the EUA declaration is terminated and will no longer be in effect. Once terminated, the unapproved product or unapproved use for an already approved product will no longer be valid to use until it receives the standard approval from the FDA.
Point of Care Tests with EUAs See the link to access a full list of tests with an EUA. Those that can be performed at the point of care will have “W” in the authorized setting column. In addition to tests that can be performed at the point of care by pharmacists, there are also tests available over the counter. Pharmacies can consider this as an option based upon supplier availability. See the links below to access CDC guidance on testing at the point of care:
See the link below for more information on at-home OTC testing:
Tests with Revoked EUA Tests that have had their EUA revoked should no longer be used or distributed for COVID-19 testing. Prior to using or recommending any COVID-19 tests, ensure that it's authorization is still current.
Clinical Laboratory Improvement Amendments (CLIA) Classification of Tests and Lab Certifications Clinical Laboratory Improvement Amendments (CLIA) are inspection standards that apply to all clinical laboratory settings regarding quality control, proficiency, and personnel. When a clinical test is evaluated for approval by the FDA, it is assigned a designation based upon its complexity. Moderate and high complexity tests can only be performed in laboratories that meet the associated CLIA requirements. However, a low complexity test is waived from these requirements. Waived tests are those which are simple to perform and do not have a high risk for incorrect results. Waived tests can be performed in non-laboratory settings that receive CLIA certificates of waiver. Point of care is not synonymous with waived tests. There are higher complexity tests that are capable of being performed at the point of care due to advancing technology. However, only waived tests can be performed outside of CLIA certified laboratory settings. In North Carolina, pharmacists are permitted to perform CLIA waived tests by the Board of Pharmacy. These tests must be FDA approved and are typically low complexity tests that can easily be performed at the point of care. Currently, the FDA is granting Emergency Use Authorizations to allow both diagnostic and serology tests to quickly be put to use during this pandemic. Under HHS guidance, pharmacists are able to perform any test that is authorized for CLIA-waived settings provided they have a CLIA waiver in place. Pharmacists can consider offering diagnostic and/or serology testing. Diagnostic tests can detect the presence of the virus, while serology tests can detect antibodies that may indicate immunity to the virus. The expansion of pharmacy services to include COVID testing offers substantially more options to patients by leveraging the position of pharmacists as one of the most accessible healthcare professionals. A CLIA certificate of waiver is necessary for pharmacists to participate in any form of onsite testing. It is important to follow all of the test manufacturer’s guidelines and parameters, as the CLIA waiver only applies if this guidance is followed. It is possible for pharmacies to partner with laboratories in order to collect specimens for higher complexity testing. In that scenario, the pharmacy does not need a CLIA waiver because no actual testing is occurring onsite. The pharmacy acts strictly as a specimen collection location. Additional information about CLIA waivers can be found here: (https://www.cdc.gov/clia/test-complexities.html)
How to Get a CLIA Waiver Fill out CMS 116 and send to NCDHHS at: NORTH CAROLINA DEPARTMENT OF HEALTH AND HUMAN SERVICESDivision of Health Service Regulation/CLIA Certification 2713 Mail Service Center Raleigh, NC 27699-2713 (919) 855-4620 FAX: (919) 733-0176 Email: [email protected]
The CMS 116 form can be found at the following link:
For more guidance on how to complete a CMS 116 form, watch the following video: An example of a complete CMS 116 form can be found at the following link: Additional CLIA waiver guidance and best practices: |